Welcome to episode 440 of The Whole View! This week, Stacy and Sarah discuss the mRNA vaccine technology in the history of vaccines. Sarah breaks down the science behind how and why vaccines work and even dispel a few myths about the new Covid-19 vaccines.
If you enjoy the show, please review it on iTunes!
The Whole View, Episode 440: COVID-19 Vaccines Part 1 – mRNA Vaccine Technology
Welcome back to episode 440 of the Whole View. (0:27)
Stacy explains that today’s topic is one she and Sarah have received the most questions on possibly ever.
Stacy also lets the audience know that this show will be a 2-parter, possibly a 3-parter depending on how deep in they get.
This show has been long in the making because she and Sarah had to wait for the research publication. Then Sarah has done her own research on top of it to prepare for this show.
Sarah shares that she’s been following this topic for about a year now: ever since the novel coronavirus was sequenced.
It’s important they lay out the science for listeners, look at the technology and history of vaccines, answer the frequently asked questions, and bust the myths surrounding this topic. (2:08)
She and Stacy decided to divide the show into multiple parts to take their time and do the subject justice.
Stacy takes a minute to address how polarizing the word “vaccine” can be. And she and Sarah are aware of this.
She wants to assure listeners they understand vaccines are a personal decision for everyone, just like every other health and medical choices are.
Stacy and Sarah are here to provide the information you need to be an informed consumer.
Note On Vaccines
In this episode, they will discuss the mRNA vaccine technology in the history of vaccines. (2:40)
In next week’s episode, Sarah and Stacy will go over the safety and efficacy data for the first two vaccines, Emergency Use Authorization, the Pfizer/BioNTech vaccine, and the Moderna vaccine.
Sarah and Stacy will discuss their thoughts on vaccinations going forward. But Stacy reminds listeners that it’s never aimed at telling others what to do.
She also reminds listeners that she and Sarah are not medical professionals.
If you have questions regarding the vaccine for yourself or your family, discuss them with your doctor.
There is a lot of information that is both true and not true floating around on the web.
Stacy is very excited to talk about the science and breakdown behind these vaccines and gives a little background on herself for context.
Both Stacy and her mother have anaphylactic reactions to things like gluten due to multiple autoimmune disorders.
Stacy has brought up to Sarah whether or not she thinks getting the vaccine is a good idea for someone with health issues like Stacy’s mom.
Stacy also wonders how having the coronavirus, but not having the antibodies, will affect her if given the vaccine.
Listener Questions
Sarah reiterates just how many questions they’ve received from listeners around this subject. (5:10)
She takes a moment to share a few she thinks accurately sum up what they want to cover in this episode.
Mae wrote:
I am sure you don’t want to cover this topic, but you are a source I highly trust as I am sure a lot of your other followers do. Would you consider doing a show about the Covid vaccines out there? It’s so hard to know what to believe these days…..Not looking to be told what to do, but merely to be presented the information as you do so well in breaking down the real science that is not filtered through such a biased lens.
Meghan added:
Can you please do an episode explaining the science behind vaccines, and explaining how they really work, including the new Covid one. You always do an excellent job of explaining things well in a relatively easy to understand way without shortcutting good science.
Stacy assures listeners that they will do their very best to break everything down.
However, you might still have questions or have heard something different that might conflict with prior information.
Stacy encourages you to reach out via the contact forms on the website for any follow-up.
If you’re part of the Patreon family, use direct access to talk with Sarah and Stacy there.
She also encourages listeners not to attack the topic on social media or to put too much emphasis on things you hear without any sources cited.
A Brief History of Vaccine Technology
Sarah starts off by going way back into the history of vaccines. (8:27)
The very first form of inoculation was called variolation.
The first variolation for smallpox dates to the 1600s in China and Ottoman Empire and practiced first in Britain and colonial Massachusetts in 1721.
They took the pus from someone suffering a natural smallpox infection. And then they’d would then rub it onto punctured or cut skin of someone who had never been exposed.
If the procedure didn’t kill you, you’d have immunity to the illness. However, Sarah noted it was pretty successful in terms of early inoculation.
Sarah explains briefly how cell memory aids in fighting episodes of re-exposures.
This is what gives us immunity or less a severe immune response when exposed.
Development Of A Smallpox Vaccine
Dr. Edward Jenner is considered the founder of vaccinology in the West.
He noticed many milkmaids were immune to smallpox. He realized they were getting infected with cowpox (a related variola virus that is relatively harmless to humans), and the infection built an immunity to smallpox.
In 1796, he inoculated his gardener’s 8-year-old son by variolating cowpox pus from a milkmaid’s hand.
Jenner then demonstrated this immunity to smallpox by exposing the boy to smallpox 6 weeks later, and he didn’t get sick.
That’s a lot of confidence! And also, not cool.
Jenner then repeated this experiment multiple times over a couple of years with different people and published his methodology in 1798.
He named his process vaccination because the cowpox virus is called vaccinia.
Doctors started administering this as a smallpox vaccine all over the world in 1798.
This is the first instance of understanding that exposing the body to a weaker version of a virus could stimulate enough of an immune response to tricker cellular memory.
Over the 18th and 19th centuries, systematic implementation of mass smallpox immunization culminated in its global eradication in 1979.
It took just about 200 years from the start of this vaccine to the eradication of smallpox.
Other Vaccine Development
Louis Pasteur’s experiments spearheaded the development of live attenuated cholera vaccine in 1897. And then an inactivated anthrax vaccine in 1904.
Plague vaccine was also invented in the late 19th Century.
Between 1890 and 1950, bacterial vaccine development proliferated, including the Bacillis-Calmette-Guerin (BCG) vaccination, which is still in use today.
In 1923, Alexander Glenny perfected a method to inactivate tetanus toxin with formaldehyde.
The same method was used to develop a vaccine against diphtheria in 1926.
Pertussis vaccine development took considerably longer, and a whole-cell vaccine was first licensed for use in the US in 1948.
mRNA vaccine technology
Sarah tells the audience that many of the childhood vaccines given to children today were developed 70 – 100 years ago.
There have been advancements in the vial today that are different from what was in the vial back then.
However, the vaccine technology is pretty much the same now, and it was that then.
Sarah underlines that mRNA vaccine technology was one of the biggest advancements since Jenner and Pasteur’s experiments.
Modern Vaccines
When looking at vaccines today, they all have the same basic ingredients (18:20)
They all work by stimulating an immune response against what’s called an antigen. An antigen is a bad thing that makes us sick.
The body develops immunological memory by the adaptive immune system in response to the antigen.
It’s the same way our immune system develops memory when we’ve been naturally infected.
But because vaccines use weaker viruses, it goes without the danger of natural infection.
Vaccinations are very costly and big investments to undertake. So we really only develop vaccines against illnesses that are very, very bad and have a huge impact on society.
Up until now, mRNA vaccine technology hasn’t changed much since the 50s.
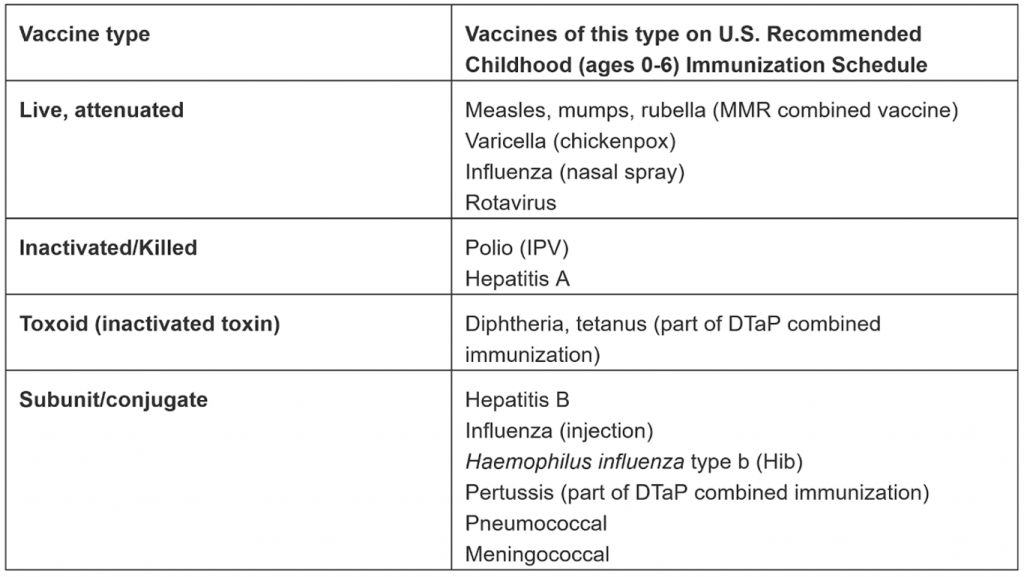
Traditional vaccines contain three components: antigen, adjuvant, and additives to preserve/stabilize.
1. Antigen
This is the thing we’re developing immunity against.
Antigens come in various types: live, attenuated virus; inactivated virus; inactivated toxins for bacterial diseases where toxins generated by the bacteria cause the illness; or parts of a virus-like split, subunit, or conjugate.
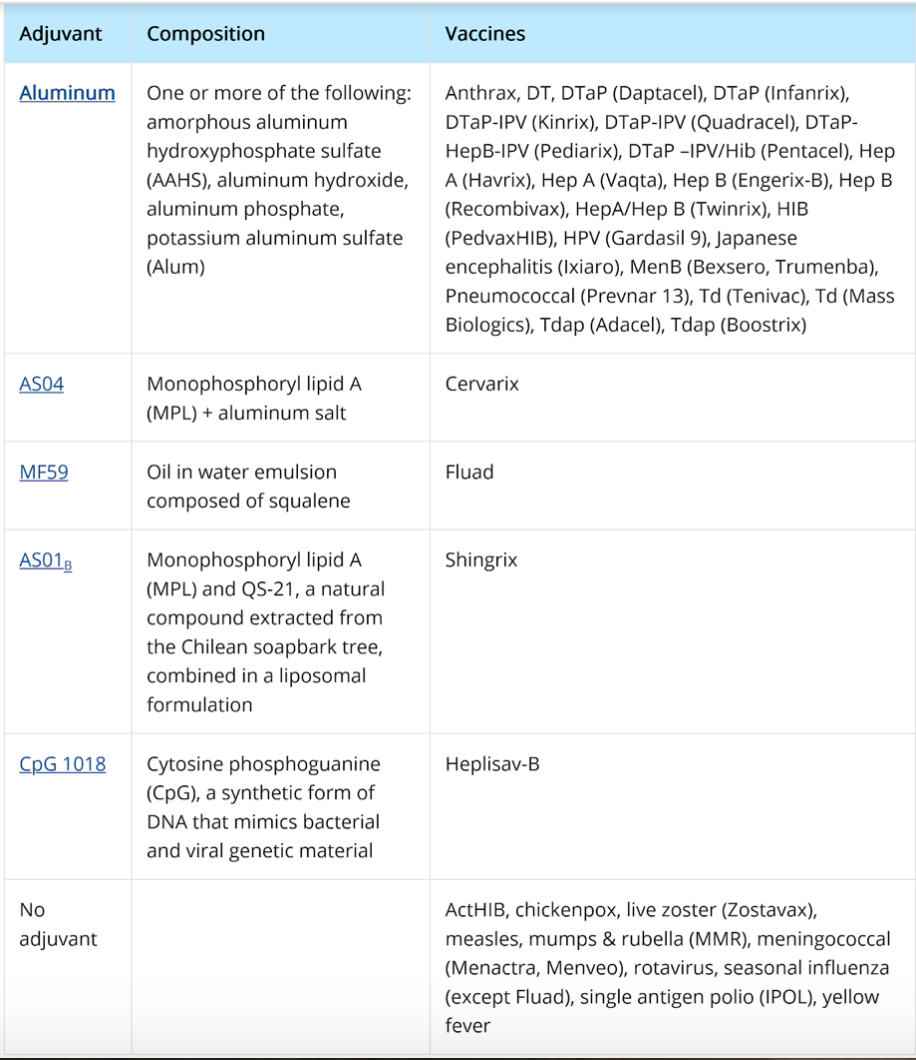
2. Adjuvants
Stacy asks about adjuvants and what they do to cause the stimulation. (20:00)
Sarah explains that adding a little bit of dead virus to our arm tissue isn’t usually enough to trigger an immune response.
An adjuvant is a compound (most commonly aluminum) that stimulates the immune system. And helps to develop a more robust immune response and stronger immunity against the antigen.
Adjuvants are why people often feel sick after a vaccine. It’s not the virus causing the side effects, but rather the ramped-up immune system caused by the adjuvant.
It’s also why many people with autoimmune diseases experience a temporary flare after vaccination.
If you already have an immune system in overdrive due to an autoimmune system, it makes sense why autoimmune suffers would have more adverse reactions.
Sarah feels it’s important to note there is no science showing vaccines cause autoimmune diseases. However, because they’re meant to cause an immune response, vaccines can make autoimmune diseases more noticeable.
Sarah recommends this article as a source of more information about adjuvants.
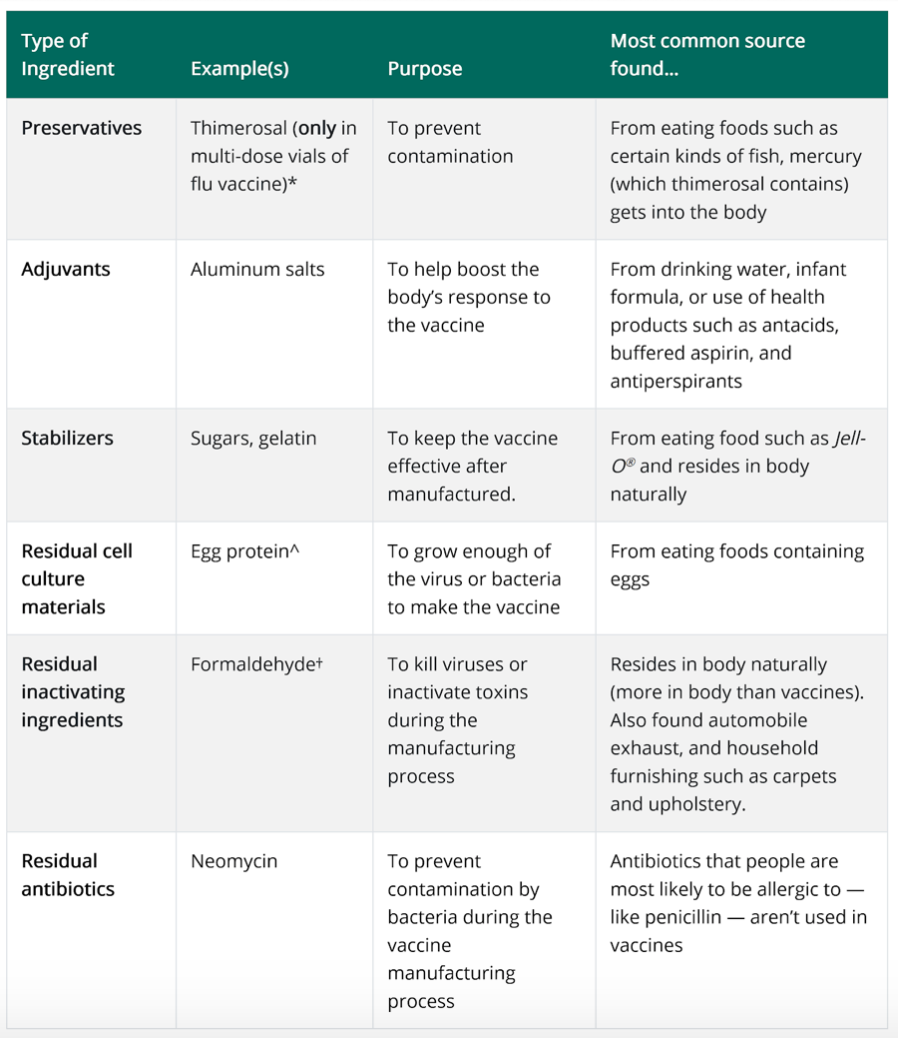
3. Additives
Additives are preservatives, stabilizers, and residuals included in the vaccine.
Sarah explains this is where there can sometimes be egg protein as a residual. So there are certain vaccines out there that people with egg allergies can’t have.
Sarah notes there is still one vaccine out there that uses Thimerosal as a preservative.
But it has been mostly phased out since the 1980s. This is because Thimerosal contains traces of mercury.
Stacy circles back to heavy metals and how often they talk about those as being bad.
She feels it’s important to note that going through normal daily life, we encounter things like heavy metals in food and water.
This is why we have livers: so we can flush them out of our systems naturally. It’s why she and Sarah talk so much about taking care of our liver.
So when we hear things like, “there’s aluminum in this vaccine,” it might come off as a red flag. We don’t want to put that in our bodies.
Stacy explains why these vaccines work to achieve the response it needs because you’re right: your body does not want that aluminum in there.
So it gets agitated and works a little bit harder to flush it out. And that’s how the vaccine can create the body’s immune response.
Stacy shares one way she helps her body is to take extra care of her liver the weeks before getting a vaccine.
That way, she could optimize her body’s ability to flush out the substances it doesn’t want in there.
Sarah agrees that a great practice is to practice self-care, such as getting enough sleep and eating right before and after getting a vaccination.
Always a Cost-Benefit Analysis
Sarah explains that Stacy brought up a great point: there is always a cost-benefit to mRNA vaccine technology and other types of vaccines. (28:45)
Sarah believes we are at a point now where most of us are disconnected from the actual impacts of viruses like polio and whooping cough.
She shares that her grandfather survived polio when he was 14-years-old. He was wheelchair-bound for 2 years and walked with a cane or walker for the rest of his life. He also developed post-polio syndrome in old age, which caused heart failure.
For Sarah, she is at the tail-end of people’s age with a personal connection with some of these illnesses that we heard about.
Gen X and younger generally don’t understand a lot of the consequences that come with a lot of these diseases.
Over a century ago, the infant mortality rate was over 20%. And the childhood mortality rate before age five was an additional disconcerting 20%.
That’s what vaccination has been able to do for us and society: give us more than a near 50% chance of reaching our 5th birthday.
We only invest in vaccines for diseases with high mortality and/or morbidity.
Sarah explains that mortality equals death.
Morbidity, on the other hand, anything bad that happens that’s not death. It includes severe illness, complications, and lifelong health problems.
For example, morbidity from mumps is basically zero. But 1 in 300 get encephalitis (or brain inflammation) while 1 in 10 men get orchitis (testicle inflammation)
Measles mortality is 1 in 500, blindness is 1 in 500, encephalitis is 1 in 1000, and pneumonia is 1 in 20.
So vaccinations aren’t just reserved for high-mortality diseases, but also ones that have a high rate of complications that can impact the quality of life long-term.
Safety Of Vaccine Technology
Safety standards are much higher for vaccines than most medications because we give vaccines to healthy people.
Some of this was learned the hard way.
For example, in April 1955, more than 200,000 children in five Western and mid-Western USA states received a polio vaccine in which was basically a bad batch.
The process of inactivating the live virus proved to be defective, so rather in inoculating the children from polio, it ended up giving them polio instead.
Within days there were reports of paralysis, and within a month, the first mass vaccination program against polio had to be abandoned.
This became a huge issue in the medical community. And it ended up enacting a lot of change in terms of what was acceptable safety standards.
Sarah explains that now vaccine technology is at the safest point it’s ever been. But there is such a thing as vaccine-induced injury.
Vaccine-Induced Injury
Stacy thinks the realities of the few cases of negative outcomes of vaccines need to be explored. (34:35)
Especially since they risk being taken out of context or misunderstood.
She wonders what Sarah knows about the frequency of these negative outcomes. And what the science sense about the risk of injury.
Sarah explains this is extremely well-tracked and well-studied.
The phenomenon of vaccine-related injury is incredibly rare. But she explains we do need to acknowledge it exists.
She attributes social media for taking these few and far between cases and inflaming them in public.
This, in turn, has destabilized a lot of the trust the public has in vaccines, which can be very harmful.
She explains that an adverse reaction is usually something like soreness near the injection site or a bruise, maybe a headache, or anything that doesn’t feel normal.
A serious adverse reaction is something that requires medical care and could potentially result in death.
Because of this risk, Sarah believes it’s very important to be aware of serious adverse reactions to ensure you’re making decisions that are medically in your best interest.
Sarah takes a few moments to summarize some of the more serious adverse reactions from commonly administered vaccines and the odds of experiencing one.
Stacy feels it’s super important to address the elephant in the room. And there is no science showing any sort of link between vaccines and autism.
Adverse reactions can occur from vaccination, but a huge amount of scientific information has really conclusively shown autism is not one of them.
For more on Vaccine-Induced Injury, Sarah recommends checking here for additional information.
Vaccine And Autoimmune Diseases
Stacy explains that in autoimmune diseases, we often see them “activate” due to an immune system flare up- for example, during pregnancy or nursing.
This isn’t to say that pregnancy or nursing caused the autoimmune disease. But rather, it triggered it to activate, and that’s why we start noticing the symptoms around that time.
She explains that this holds true with vaccines as well.
If someone starts to notice autoimmune systems after receiving a vaccine, that vaccine itself didn’t “cause” the immune disease.
Rather, it agitated the immune system. And that agitation triggered the symptoms of an autoimmune disease that was already lying latent inside the body.
Sarah adds there’s no evidence saying people with autoimmune diseases should avoid vaccines.
If anything, they may need more booster vaccines to reach adequate immunity due to the immune system already not functioning optimally.
The Importance Herd Immunity
Sarah also reminds listeners that vaccines aren’t actually about individual protection at all. (46:10)
They protect you individually, sure, but the reason vaccines are so amazing (and why smallpox was able to be eradicated) is because of the creation of herd immunity.
Herd immunity means enough of a community is immune to an illness (cannot get it and cannot pass it) that if there is an individual infection, the illness has nowhere to go. It’s stuck.
Herd immunity limits the path for the virus to spread and can be much more easily contained.
Herd immunity also protects members in our community who might have some sort of medical issue that prevents them from being vaccinated themselves.
Sarah cites children with cancer are unable to get vaccinated due to their health issues.
So being surrounded by people who cannot spread a life-threatening illness is very beneficial to their health and wellness.
Smallpox, which had an incredibly high mortality rate and permanent scarring, no longer exists anywhere in the world because of vaccines!
So while we might want the covid vaccine for individual protection, that’s not the primary goal. The primary goal of vaccination is community protection.
How mRNA Vaccines Work
mRNA vaccines are the biggest advance in vaccine technology since Louis Pasteur and Edward Jenner. (50:35)
It can revolutionize not just immunizations but also cancer therapy and other drug development.
Brief History of mRNA Vaccine
mRNA stands for messenger RiboNucleic Acid.
Our cells make as an intermediary between the DNA in our cell’s nucleus and a protein.
It also functions as a set of instructions to make protein, which is the intermediate step between DNA and the protein it encodes
The steps are: DNA – transcription -> RNA – translation -> protein
Translation may occur at ribosomes free-floating in the cytoplasm. Or directed to the endoplasmic reticulum by the signal recognition particle.
mRNA was first discovered in 1961 by Sydney Brenner at Cambridge and James Watson at Harvard.
The concept of mRNA-based drugs occurred in 1989 when Malone demonstrated that mRNA could be successfully transfected and expressed in various eukaryotic cells under a cationic (positively charged) lipid package.
In 1990, in vitro-transcribed mRNA was sufficiently expressed in mouse skeletal muscle cells through direct injection. This became the first successful proof of the feasibility of mRNA vaccines.
After the first mRNA-based drug company was established in 1997, many groups began to research and develop mRNA-based drugs.
So far, over twenty mRNA-based candidate drugs have entered the clinical trial stage.
A big advance in 2005 when Katalin Karilo and Drew Weissman at the University of Pennsylvania showed how to modify mRNA to get into human cells without triggering an immune response.
Major advances in lipid nanoparticle technology for the mRNA envelope over the last 4-5 years.
Last 4-5 years, improvements in mRNA vaccines increase protein translation, modulate innate, adaptive immunogenicity, and improve delivery.
This mRNA vaccine technology has been perfected in just the last few years.
This is why the Covid-19 vaccine was able to be developed so quickly. The technology we needed to create this vaccine was already primed and ready to go.
How Do mRNA Vaccines Work?
Sarah explains that the coolest part of mRNA vaccine is that they do not use adjuvants! (58:01)
This is because adding the RNA to the cell nucleus is enough to trigger it to replicate. It doesn’t need anything additional to trigger the immune response.
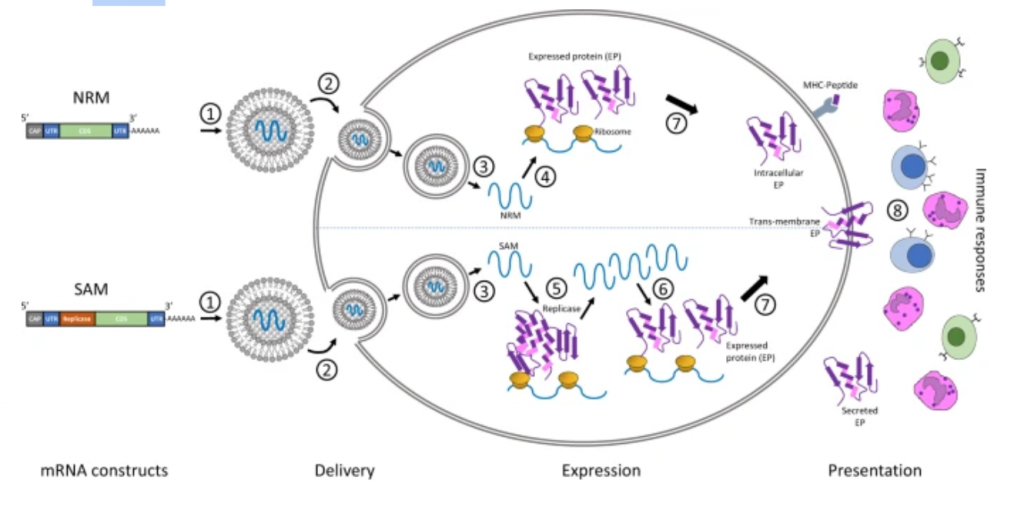
Two major types of RNA are currently studied as vaccines:
- non-replicating mRNA
- which is what’s in both the Pfizer/BioNTech covid-19 vaccine and the Moderna covid-19 vaccine
- virally derived, self-amplifying RNA.
Conventional mRNA-based vaccines encode the antigen of interest and contain 5′ and 3′ untranslated regions (UTRs).
Self-amplifying RNAs encode the antigen and the viral replication machinery that enables intracellular RNA amplification and abundant protein expression.
The lipid envelope facilitates entrance into the cell via endocytosis and exit from endosome into cytoplasm
This molecule provides the template in the cytoplasm of a cell for translation by the ribosome.
And tRNA into the encoded protein, making multiple copies of the protein from each mRNA template.
The protein can then be presented to the immune system through MHC or, like both Pfizer/BioNTech and Moderna vaccine, the protein is transmembrane, so it presents itself!
Sarah explains that there were some human trials using mRNA vaccines to treat cancer patients.
So yes, as Stacy brings us, the technology is still pretty new.
But this isn’t the first time we’re using mRNA technology. It’s the first opportunity we’ve had to utilize the discoveries large-scale.
Ingredients Of mRNA Vaccines
Sarah explains that what makes this new vaccine technology so cool is how few ingredients it requires to make. (1:05:20)
- mRNA (rather than a live attenuated virus, dead virus, or split virus)
- Lipid nanoparticle envelope (rather than viral particles floating around a solution or viral vector-like adenovirus)
- LNPs often consist of four components:
- an ionizable cationic lipid, which promotes self-assembly into virus-sized (~100 nm) particles and allows endosomal release of mRNA to the cytoplasm;
- lipid-linked polyethylene glycol (PEG), which increases the half-life of formulations;
- cholesterol, a stabilizing agent;
- and naturally occurring phospholipids, which support lipid bilayer structure.
It requires no adjuvant, which is SO COOL!
Adding an adjuvant to the lipid envelope has been studied, but it doesn’t seem to be necessary.
This is because foreign mRNA and viral proteins are really good at eliciting an immune response.
- mRNA has self-adjuvant properties which activate strong and long-lasting adaptive immune responses through tumor necrosis factor-α(TNF-α), interferon-α(IFN-α), and other cytokines secretion by immune cells
- The foreign viral proteins are presented via MHC-I
Lipid nanoparticles may have a little adjuvant activity in some circumstances. But basically, all of the immune stimulation is targeted against the foreign viral protein and mRNA!
For example, here are all the ingredients for the Moderna Vaccine:
- The vaccine contains a synthetic messenger ribonucleic acid (mRNA) encoding the pre-fusion stabilized spike glycoprotein (S) of SARS-CoV-2 virus.
- lipids (SM-102, 1,2-dimyristoyl-rac-glycero-3-methoxypolyethylene glycol-2000 [PEG2000-DMG], cholesterol, and 1,2-distearoyl-sn-glycero-3-phosphocholine [DSPC]),
- pH Buffering agents: tromethamine, tromethamine hydrochloride, (both drugs for metabolic acidosis) acetic acid, sodium acetate, (both naturally found in our blood)
- Cryo-stabilizer: sucrose
Sarah jokes about how much she’s nerding out about it.
Advantages
Over the past decade, major technological innovation and research investment have enabled mRNA to become a promising therapeutic tool in vaccine development and protein replacement therapy.
The use of mRNA has several beneficial features over subunit, killed, live attenuated virus, and DNA-based vaccines.
1. Safety
As mRNA is a non-infectious, non-integrating platform, there is no potential risk of infection or insertional mutagenesis.
Additionally, mRNA is degraded by normal cellular processes. And it’s in vivo half-life can be regulated through the use of various modifications and delivery methods 9,10,11,12.
The inherent immunogenicity of the mRNA can be down-modulated to further increase the safety profile9,12,13.
2: Efficacy
Various modifications make mRNA more stable and highly translatable9,12,13.
Efficient in vivo delivery can be achieved by formulating mRNA into carrier molecules, allowing rapid uptake and expression in the cytoplasm (reviewed in Refs 10,11).
mRNA is the minimal genetic vector; therefore, anti-vector immunity is avoided, and mRNA vaccines can be administered repeatedly.
mRNA vaccines expressing antigen of infectious pathogen induce both strong and potent T cell and humoral immune responses
Even better for viruses requiring cellular immunity like coronaviruses. (Click here for more!)
3. Production
mRNA vaccines have the potential for rapid, inexpensive, and scalable manufacturing, mainly owing to the high yields of in vitro transcription reactions.
They are really fast to make. Moderna took 2 days to create the RNA sequence to produce the spike protein after sequencing the virus genome in January.
Then shipped its first vial of vaccine to NIH for trials 41 days after that.
This will also mean the vaccine can be modified for new strains (so far, not necessary), and we can get a vaccine even faster in the event of another pandemic!
Myths About the mRNA Vaccines
One of the biggest myths many people believe is that the vaccines were rushed. So we don’t know if they’re safe. (1:07:30)
The unprecedented investment (funding) allowed for tests normally done serially to be done in parallel. And it allowed for manufacture (normally 6 months to a year) to be done during clinical trials rather than after.
These vaccines build upon vaccine research from SARS and MERS and the knowledge base about coronaviruses from that research.
So we’ve been researching it longer than people have known about the novel coronavirus.
For example, it was already known that the spike protein bound with ACE2. And that’s how SARS-CoV-2 infects cells.
It also builds upon a tremendous amount of mRNA vaccine research and clinical trials of mRNA vaccines for cancer.
mRNA vaccine technology allows for a fast process. It’s also very inexpensive to make. Yay science!
Vaccines have some of the most stringent safety standards in all of pharmaceutical development!
They are given to healthy people, not sick, so tolerance for serious reactions is lower. Also, these vaccines were tested thoroughly and have exceeded the standards.
No corners were cut!
Yes, there are still some things we don’t know (like whether or not you can get an asymptomatic case after you’ve been vaccinated and then spread the virus or how long immunity will last), but we do know that the safety profile is excellent.
It’s approved for 16 and over because they did tests on adults before children. In fact, the 12-15 age groups are being tested now.
Final Thoughts
One of the biggest reasons these vaccines were able to be produced so fast is because of the timing. (1:10:42)
Scientists have been working on vaccine technology for centuries. And major advancements in the last 30 years have made it possible to produce both efficient and safe vaccines.
This is why basic science funding is so, so important.
Sarah goes into why this basic funding is so important. Most funding is going to direct human relevance.
The science that these vaccines are based on comes down to a basic discovery and expanding human knowledge.
And only after the fact, we understood how it could be applied to improving human life.
So increasing funding for basic science discovery is very important to Sarah.
Stacy also circles back to how mind-blowing that this basic science discovery could also further our advancement toward a cure for cancer.
She reminds listeners that there are two vaccines approved for disruption in the US.
Next week, Sarah and Stacy with dive into the science and myths on those to bring you all the info you need to make your own decision.
If you’re curious how Sarah and Stacy really feel about this topic, pop on over to Patreon for more science talk and bonus content.
See you next week!